by: Brett Windsor, PT, PhDc, MPA, OCS, FAAOMPT
Today’s post, and the next 3-4 posts, are focused on the total management of the orthopedic physical therapy patient. Effective management necessarily relies on a preceding thorough and accurate evaluation and diagnosis; we’ve discussed those issues recently. Nevertheless, there is a rhythm and a structure that can be given to the management process that fits with the eclectic philosophy that is NAIOMT – everything works some of the time, nothing works all of the time…knowing what is really wrong maximizes the chances of an effective management program tailored to each individual patient who is cognizant of their role in the overall process.
Management begins and ends with education…in fact…it’s incredible, perhaps more so as clinical experience accumulates, how often education is the only treatment needed. Techniques are great; it’s nice to ‘fix’ something. More and more though, time spent deeply educating our patients is profoundly effective – it provides patients with the understanding of their problems essential to ensuring the ability to own their problem and work with PT to facilitate a return to optimal movement patterns and function. Once evaluated and diagnosed, education begins in earnest. Education proceeds through three phases. Also, it should go without saying that every patient should be screened for lifestyle risk factors such as smoking, nutrition and obesity; these can have a profound effect on symptoms and render PT largely ineffective if not dealt with in PT, or in partnership with other qualified health professionals.
Firstly, educate about diagnosis. Each patient should have a full and complete understanding of exactly what is wrong with them and how that has lead to the presenting symptoms. This holds true for the simplest ankle sprains through to the most complicated chronic pain states. When patients understand why, there is a deeper connection and willingness to adhere to management programs that might not seem intuitive. Secondly, educate about prognosis. Patients should understand how their condition will progress over time with no management and also comprehend how recovery should progress with management, in light of their individual circumstances. Finally, educate about the management plan – not only the specific tools and techniques on offer, but the relative contributions of the physical therapist, and the patient. The full process can take minutes, or, a few sessions, depending on complexity.
Next, activity modification takes place. Its simplest focus is what the patient does all day every day, offering optimal methods of positioning, of moving, of recreating, and of resting. What hurts should be minimized – disc patients should avoid sitting as much as possible – what doesn’t hurt should stay….to a point. Understanding pathology and biomechanics helps, a lot. For instance, the stage of healing of a disc will largely determine not only the positional preferences of the patients postures and activities, but also the length of time any one position should be sustained. Stenotic patients will receive advice tailored to their circumstances, as will the ‘unstable’. Manual therapy techniques and tools will make absolutely no difference if exquisite attention to detail is not paid to the postures, positions, movements and activities of daily life. Again, sometimes it’s relatively easy to do this, other times it’s not.
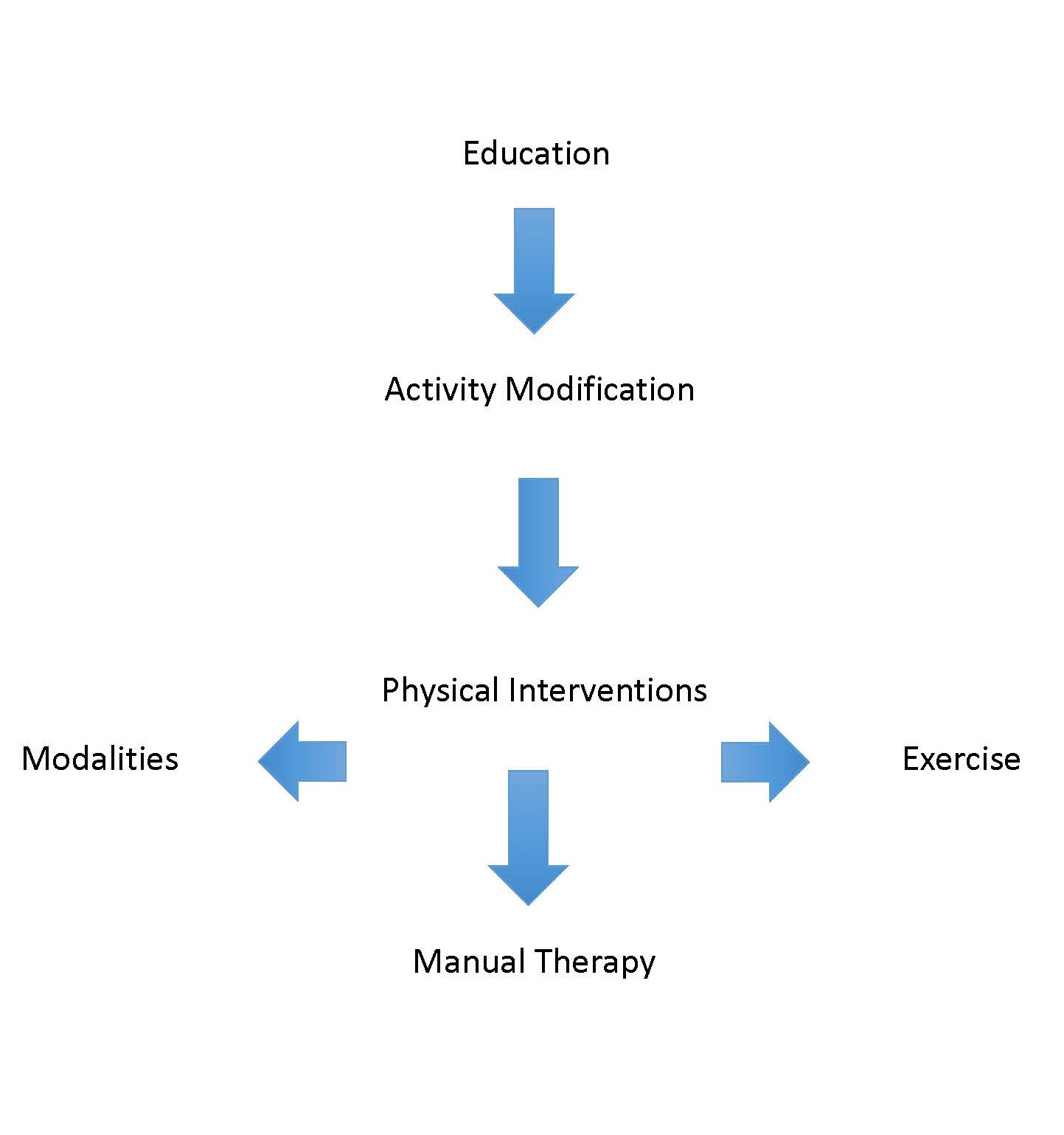
Finally, physical interventions. Every intervention physical therapy has to offer fits into one of three categories – manual therapy, exercise, or modalities. Many interventions may cross categories – for example, is dry needling manual therapy or a modality? What about kinesiotape? At any rate, what ever you can think of in terms of intervention…mobilization, manipulation, muscle energy, strain-counter-strain, ASTYM, Graston, taping, stabilization, Pilates…all have at least one home. Remember, everything works some of the time…and there’s much more out there than just manual therapy. In general, we know that manual therapy and exercise work well together. Increasingly, evidence supports a neurophysiological mechanism for manual therapy, so it is beneficial to offer corrective exercise immediately after any manual therapy technique to ensure new movement patterns are consolidated. Then PT avoids the passive reapplication of techniques over a long period of time. As a general rule, there is little evidentiary support for modalities, but anyone who has been in clinical practice for a while knows that they have their place.
So there you have it….this is one way among many ways to approach management. Hopefully this structure provides a basis for the contention that management of physical therapy patients is about so much more than just a manual therapy fix. Manual therapy is of course an important part of the management plan; NAIOMT and others like us wouldn’t exist if it didn’t play a vital role. But, as time goes on…education and modification of an individuals daily pursuits (education based a well) are seemingly the absolute keys to long-term recovery…with a parallel focus on lifestyle factors and general wellness incorporated. And really, who is better placed to provide this type of management than a physical therapist?
We’d love to hear your thoughts and comments on this topic…
Our next post will focus on a real-life patient example…one where education played a critical role in a patients long-term recovery…


Dr. Windsor,
I have been following the NAIOMT blog post for a month now, and have enjoyed reading all the writings. I am relatively new to the NAIOMT system, but have trained in various philosophies in manual therapy. I have not found any system of evaluation to be the best blend of everything from ,the medical model, patho-anatomical, and symptom based model, and a thorough curriculum in differential diagnosis, than what I have found in my training with NAIOMT. I have been a pure “McKenzie therapist” for years when I took a lot of interest in treating spine patients. I say pure only because back in 2002, there was relatively no OMPT philosophy involved. Then I found something was missing. Force progressions and alternatives when reducing or treating disc pathology and dysfunctions in flexion, extension or rotation is about applying the necessary forces accurately. The precision in applying these forces can only be learned in a curriculum that is truly ecclectic in nature.
Thanks to NAIOMT and the Andrews DSc program.
LikeLike
Thank you for your comments Andrei. I appreciate your positive words about eclecticism. It’s an important variable that certainly creates the ability to be wide-ranging in scope. Everything works some of the time…nothing works all of the time…best of luck with your studies. Best regards. Brett. P.S. Not a Dr yet…hope to be when I grow up 🙂
LikeLike
Hey there! I’ve been reading your website for some time now and finally got the bravery to go ahead and give you
a shout out from Atascocita Texas! Just wanted to say keep up the great job!
LikeLike
Thank you for that. It is very much appreciated. Best regards. Brett
LikeLike
It was refreshing to read this again; looking at the past 3 years of my career, this philosophy shaped how I practice. Thanks for instilling this in your students!
LikeLike