
Hello from Eugene, Oregon where I’ve been volunteering at the USATF Outdoor Championships!
Last year I was chosen along with a dozen or so other physical therapist’s to cover the 2014 IAAF World Junior Championships at Hayward Field in Eugene, Oregon. Like many other professionals who volunteer their time, I do it because I love my profession and feel we have much to offer our athletic population. The championship meet brought together the top 1,700 under 19-year-olds from 167 countries to compete at historic Hayward Field, the first IAAF World Junior Championship ever held in the United States. The caliber of young athletes who qualify and train for these events is exceptional. These athletes have a grueling training schedule, five to seven days a week, three to eight hours a day. With the amount of training and competition the strain on their bodies and potential risk of injury is high. I was pretty excited to help out at such an elite level. After receiving my SWAG of matching shirt, shorts and jacket, I was ready to roll.
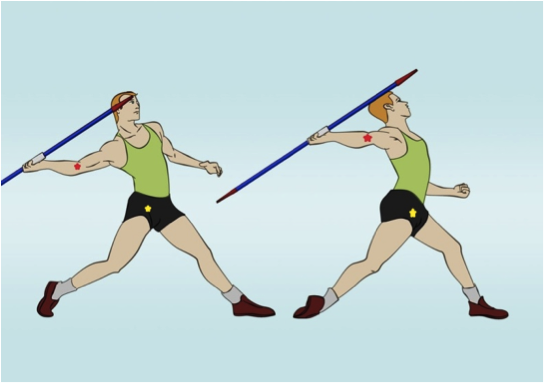
Right off the bat the first athlete that came to me presented with a groin strain. He was a 19 y/o javelin thrower with complaints of groin pain. After a quick history, I ascertained that he had this strain for over a month, secondary to a strained elbow that he had been nursing for over a period of 2-3 months. Hmm, I wonder what is causing this groin strain. If you have ever seen the mechanics of a right handed javelin thrower you will note in the final stride, the athlete plants their left leg and pushes off with their right. Simultaneously turning hips so they are perpendicular to the target area as they transfer their weight forward while bringing arm up and forward keeping elbow high.
Immediately I wanted to go into manual therapy mode and talk with him about his mechanics and how the elbow being hurt may be causing him to try and compensate with his hip and how this increased torsion can cause stress. I wondered how his thoracolumbar junction mechanics looked. And then he asked me…“Do you have ultrasound”?
What? Did he really just say that? Yes he did, the young athlete and his coach just wanted me to ultrasound the groin area.
Now, any respectful manual therapist knows we despise the referrals that note “ultrasound only”. Ultrasound is not what I want to do after spending thousands of dollars and many hours in the clinic trying to improve my manual therapy skills. I feel I have so much more to offer. Well the truth is at this level, with these kids trying to make the Olympics, the question is not how I can help this athlete in the long run. It is how I can get this athlete enough pain relief to compete today or tomorrow. Sometimes it’s ultrasound. Yes, I said it, ultrasound! That does not mean while I was getting a wrist cramp from ultrasounding every other athlete that walked into the tent, that I was not talking mechanics “to the ones who understood English”. I continued my push to discuss training and mechanics to athletes and their therapists.

PT, OCS, COMT, FAAOMPT and Paul Westgard, PT, DPT, OCS, SCS, CSCS with Eugene, a Kenyan PT at the USATF Outdoor Championships
One of the therapists was Eugene from Kenya, he had the responsibilities for the care and medical treatment for team Kenya. He enjoyed sharing duties and collaborating with us on his athlete’s needs and wants. Most of the time the collaboration came down to Ultrasound, Ice Bath, Iontophoresis and many other things that require no manual or mechanical skill at all.
Even though I did little manual therapy I still found enjoyment working with these elite junior athletes. It was exciting to be a part of such a big international event, this year I am looking forward to working with a great group of medical volunteers and see America’s top track and field athletes compete in the 2015 USATF Outdoor Championships.
So, the next time you get a request for ultrasound, maybe you can come down from that manual therapy pedestal and join me in educating our athletic population while performing this necessary evil.
-Russ Case, PT, OCS, COMT, FAAOMPT


We have the same issues with out athletic teams and patients having inc pain etc. Everyone always feels better afterwards, Placebo?
LikeLike
Great post Russ. Agree with everything you just said. I just had a patient recently who came in and the first words out of her mouth (not even kidding) were “it’s not a good day for a student” (which was rude because my student was at the tail end of her clinical and was really just trying to be kind and help this person out) and “now before I leave today I had better have ultrasound and electrical.” Now I am a pretty passionate person about what we do so both of those comments made my systolic pressure go up more than a few mmHg. I tried and tried to educate her on the current best evidence and how modalities are showing less and less clinical utility compared to other treatments but I was just hitting my head against the wall because this women was set that modalities were king in the western medicine world. I took off my “preach the best evidence” hat and put on my “it’s not about me, it’s about the patient” hat and just conceded to do modalities with the agreement that she would do a little evidenced based stuff for me. I still have a lot of resistance when I see her, but at the end of the day.. I know the evidence for modalities and I know it’s weak. But if the placebo effect gets her better faster, an outcome is an outcome in my book
LikeLiked by 1 person
I had a podiatrist yell at me because I was not doing the iontophoresis and ultrasound he had ordered (which I don’t even have in the clinic) for his patient with a two year history of plantar fasciitis… This was after he had already attempted oral anti-inflammatories and a cortisone shot over the past six months, none of which worked. She went back to him after the second visit and said I wasn’t doing what he had ordered. He screamed at me that I had no idea what I was doing and I should do what I was told. I lost it. I mean…. LOST IT.
“At what point do you stop going down the same road and try to actually look at the mechanics? Why do all these inflammatory processes exist in isolation to doctors? Do you really think the plantar fascia just decided one day to just go off the rails by itself? You hit the damn thing with cortisone and it came back. Great job shooting cortisone into soft-tissue, by the way. We all know that does wonders for tissue tensile strength.”
He hung up on me.
The patient called me back two days later and asked if she could come back in. Lo and behold, she was actually experiencing relief from the subtalar and talocrural mobilizations. I treated the patient for three more visits with manual therapy with zero modalities, and got her back to 100%.
I sent a very kind thank you note to the podiatrist for the referral. Never heard anything back.
LikeLike